Whereas, Great Leader is most durably wedded to the “Operation Chuck You, Farley” camp … 
(Washington Post, April 18, 2020):
“Contamination at CDC lab delayed rollout of coronavirus tests”
Food and Drug Administration officials concluded that the CDC violated its own laboratory standards in making the kits. The substandard practices exposed the kits to contamination.
The troubled segment of the test was not critical to detecting the novel coronavirus, experts said. But after the difficulty emerged, CDC officials took more than a month to remove the unnecessary step from the kits, exacerbating nationwide delays in testing, according to an examination of federal documents and interviews with more than 30 present and former federal scientists and others familiar with events.
(BBC, April 18, 2020):
“Coronavirus: Double warning over antibody tests”
The UK has placed antibody tests - which check if someone has had Covid-19 - at the centre of an eventual “back-to-work” plan to restart normal life. But experts said they may not prove if someone is protected from reinfection.
The UK’s testing co-ordinator has also warned people not to buy private tests. The government has already paid for three-and-a-half million antibody tests, but has not yet found one that is reliable enough to use - and stresses that it will not approve the use of any test until it can be sure its findings can be fully depended on.
(New York Times, April 18, 2020):
“Nothing like this has ever been seen in terms of the number of people needing
kidney replacement therapy,”
Yeah I hear ya, it’s like spending the day on “Wikipedia” that’s why I gave up on this thread 
1 Like
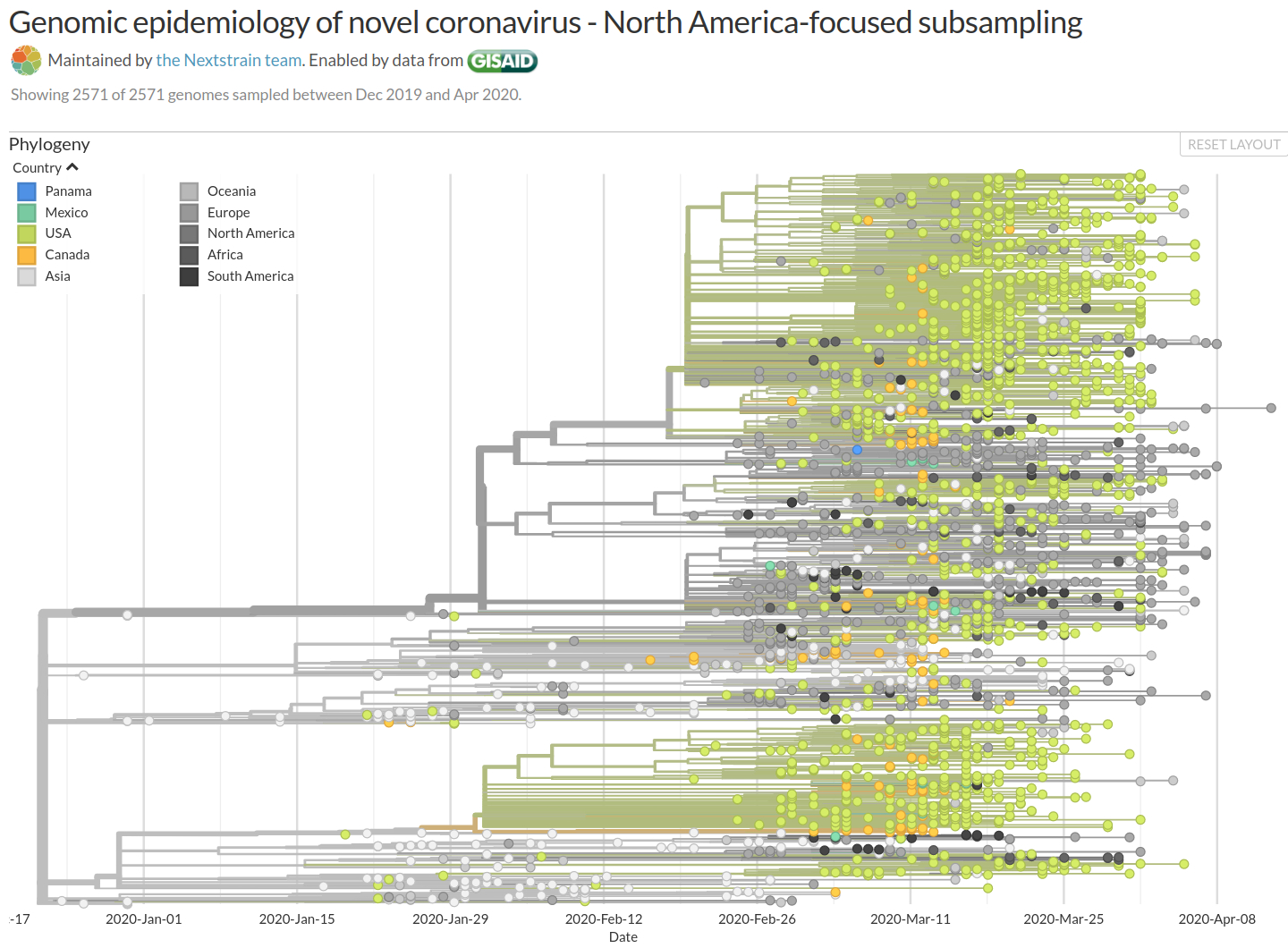
This particular data is for North America (4/18/20) variants/mutations (mouse-over identifies mutations):
(what was in this email that was posted?)
1 Like
Some important information about systemic (beyond pulmonary, lung) COVID-19 effects on the body.
(Science, April 17, 2020):
“How does coronavirus kill? Clinicians trace a ferocious rampage through the body, from brain to toes”
2 Likes
(Science Alert, April 20, 2020):
“Scientists Still Don’t Know if Recovering From COVID-19 Confers Immunity or Not”
“It is possible that the antibodies that someone develops against the virus could actually increase the risk of the disease becoming worse,” he said, noting that the most serious symptoms come later, after the patient had formed antibodies.
For the moment, it is also unclear whose antibodies are more potent in beating back the disease: someone who nearly died, or someone with only light symptoms or even no symptoms at all. And does age make a difference?
Faced with all these uncertainties, some experts have doubts about the wisdom of pursuing a “herd immunity” strategy such that the virus - unable to find new victims - peters out by itself when a majority of the population is immune.
.
(Univesity of Minnesota CIDRAP, April 15, 2020):
“Antibody tests may hold clues to COVID-19 exposure, immunity - but it’s complicated”
The question of immunity
The unknowns begin with how much an immune response to SARS-CoV-2 - the virus that causes COVID-19 - tells us. Early studies suggest the production of IgM and IgG in COVID-19 patients typically occurs between 7 and 11 days after exposure, with IgM antibodies appearing first, followed by IgG antibodies.
The presence of these antibodies, which respond to specific antigens on the surface of the SARS-CoV-2 virus, indicate that a person has been exposed and their immune system has reacted. But does that necessarily mean a person is immune to getting re-infected? “Often, but not always, the presence of antibodies corresponds to immunity to that agent, and if that turns out to be the case for COVID-19, that would be extremely important,” says Storch. …
Test accuracy is unclear
But at the moment, the true accuracy of serologic tests for SARS-CoV-2 is another unknown. So far, the Food and Drug Administration (FDA) has granted an emergency use authorization (EUA) for only one antibody test -the qSARS-CoV-2 IgG/IgM Rapid Test from Cellex. The EUA allows a company to market unapproved diagnostic and therapeutic products during a declared emergency. According to Cellex, the test was 93.8% sensitive in testing on 128 samples from Chinese COVID-19 patients confirmed by reverse transcription polymerase chain reaction (RT-PCR), and 96.4% specific.
Those impressive-looking numbers, though still leave the possibility of a significant number of people having false-positive and false-negative tests. For example, if 5% of the US population actually had the virus, a test with 95% sensitivity and 95% specificity conducted in a million people would correctly detect 47,500 cases, along with 2,500 false-negatives (those who were infected but were missed). But it would also produce 47,500 false-positives. So, if only 5% of the population was infected, the number of true-positives and false-positives would be the same.
“Imagine going to a healthcare worker and saying ‘we’re going to test you for antibodies right now, and if you’re positive, you have a 1 in 2 chance it’s not real,’” says Michael Osterholm, PhD, MPH, director of the Center for Infectious Disease Research and Policy (publisher of CIDRAP News). “Are you actually going to use that test in a meaningful way?” …
… The MDH’s Bartkus says there are currently more than 70 vendors that have notified the FDA of their intent to market antibody tests that look for some combination of IgM, IgG, and immunoglobulin A (IgA) response. And little is known about these tests. … “We’re building the plane as we’re flying it,” she says.
3 Likes
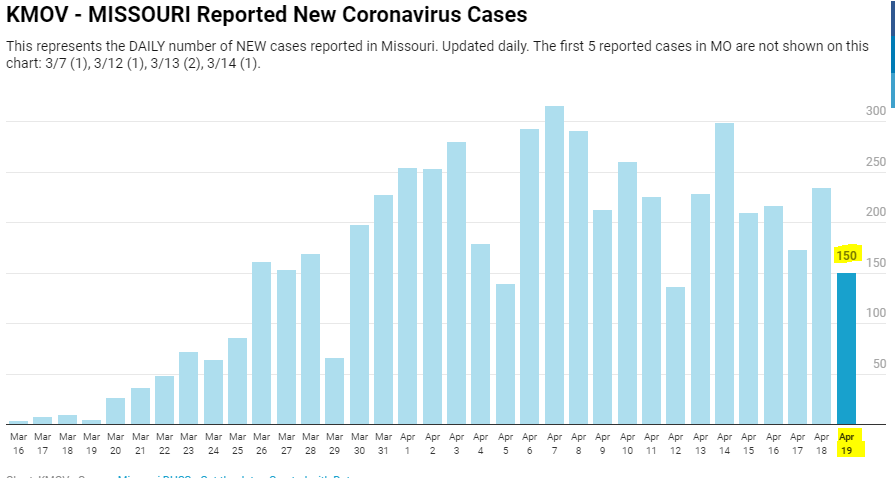
I’m not a smart man, but I did learn long ago that St. Louis is part of Missouri. So when see these numbers, my dumb really gets itchy.

3 Likes
(CNBC, April 20, 2020):
“Coronavirus antibody testing shows LA County outbreak is up to 55 times bigger than reported cases”
The Covid-19 outbreak in Los Angeles County is likely far more widespread than previously thought, up to an estimated 55 times bigger than the number of confirmed cases, according to new research from the University of Southern California and the LA Department of Public Health.
USC and the health department released preliminary study results that found that an estimated 4.1% of the county’s adult population has antibodies to the coronavirus, estimating that between 221,000 adults to 442,000 adults in the county have had the infection.
This new estimate is 28 to 55 times higher than the 7,994 confirmed cases of Covid-19 reported to the county through early April. The number of coronavirus-related deaths in the county has now surpassed 600, according to the Department of Public Health. The data, if correct, would mean that the county’s fatality rate is lower than originally thought. The results are based on antibody testing of about 863 people who were representative of LA County, the researchers said.
.
2 Likes
(New York Times, April 20, 2020):
… patients did not report any sensation of breathing problems, even though their chest X-rays showed diffuse pneumonia and their oxygen was below normal. How could this be?
We are just beginning to recognize that Covid pneumonia initially causes a form of oxygen deprivation we call “silent hypoxia” - “silent” because of its insidious, hard-to-detect nature.
Pneumonia is an infection of the lungs in which the air sacs fill with fluid or pus. Normally, patients develop chest discomfort, pain with breathing and other breathing problems. But when Covid pneumonia first strikes, patients don’t feel short of breath, even as their oxygen levels fall. And by the time they do, they have alarmingly low oxygen levels and moderate-to-severe pneumonia (as seen on chest X-rays). Normal oxygen saturation for most persons at sea level is 94 percent to 100 percent; Covid pneumonia patients I saw had oxygen saturations as low as 50 percent.
To my amazement, most patients I saw said they had been sick for a week or so with fever, cough, upset stomach and fatigue, but they only became short of breath the day they came to the hospital. Their pneumonia had clearly been going on for days, but by the time they felt they had to go to the hospital, they were often already in critical condition. …
… A vast majority of Covid pneumonia patients I met had remarkably low oxygen saturations at triage - seemingly incompatible with life - but they were using their cellphones as we put them on monitors. Although breathing fast, they had relatively minimal apparent distress, despite dangerously low oxygen levels and terrible pneumonia on chest X-rays.
We are only just beginning to understand why this is so. The coronavirus attacks lung cells that make surfactant. This substance helps keep the air sacs in the lungs stay open between breaths and is critical to normal lung function. As the inflammation from Covid pneumonia starts, it causes the air sacs to collapse, and oxygen levels fall. Yet the lungs initially remain “compliant,” not yet stiff or heavy with fluid. This means patients can still expel carbon dioxide - and without a buildup of carbon dioxide, patients do not feel short of breath.
Patients compensate for the low oxygen in their blood by breathing faster and deeper - and this happens without their realizing it. This silent hypoxia, and the patient’s physiological response to it, causes even more inflammation and more air sacs to collapse, and the pneumonia worsens until their oxygen levels plummet. In effect, the patient is injuring their own lungs by breathing harder and harder. Twenty percent of Covid pneumonia patients then go on to a second and deadlier phase of lung injury. Fluid builds up and the lungs become stiff, carbon dioxide rises, and patients develop acute respiratory failure. By the time patients have noticeable trouble breathing and present to the hospital with dangerously low oxygen levels, many will ultimately require a ventilator.
2 Likes
(The Guardian, April 20, 2020):
(Ars Technica, April 20, 2020):
As the new coronavirus took root across America, the US Centers for Disease Control and Prevention sent states tainted test kits in early February that were themselves seeded with the virus, federal officials have confirmed. …
… The CDC had been vague about what went wrong with the tests, initially only saying that “a problem in the manufacturing of one of the reagents” had led to the failure. Subsequent reporting suggested that the problem was with a negative control - that is, a part of the test meant to be free of any trace of the coronavirus as a critical reference for confirming that the test was working properly overall.
Now, according to investigation results reported by The New York Times, federal officials confirm that sloppy laboratory practices at two of three CDC labs involved in the tests’ creation led to contamination of the tests and their uninterpretable results.
Well then stop breathing and talking so much ![]()
1 Like
I think that MIT article I found addressed that. Did you see that one? Sounds like a read you would be interested in? Actually, all the MIT articles were good.
1 Like
Just happened to stumble on this one looking for birthday cards, lol. Don’t have to go far to find covid links.
1 Like