Read whatever you may choose, but the metric is accurate exactly as it has been clearly described - a measure of relative risk of death from COVID-19 infection proportional to populations residing per unit geographical areas of countries considered. (Obviously), metric is derived from averaged population densities. Relevant data (no matter how presented) does not seem to portray Sweden very favorably.
.
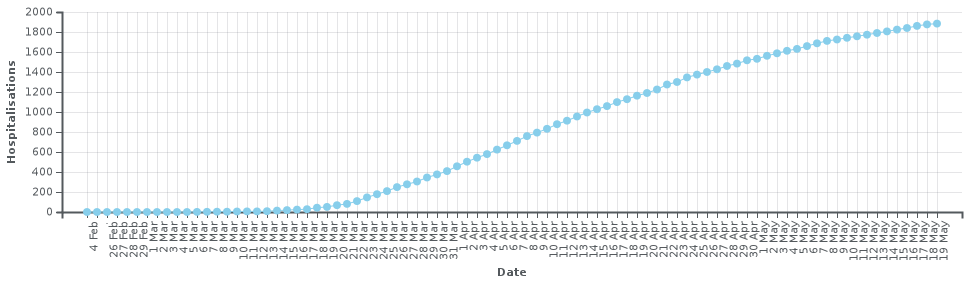
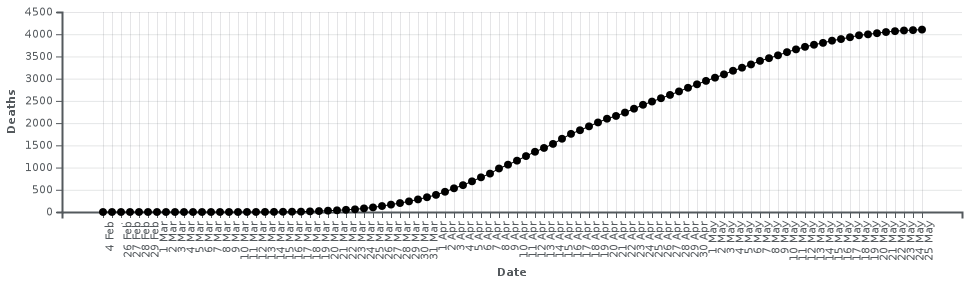
Perhaps another (not population density normalized) item on the “data smorgasbord” appeals to you ?
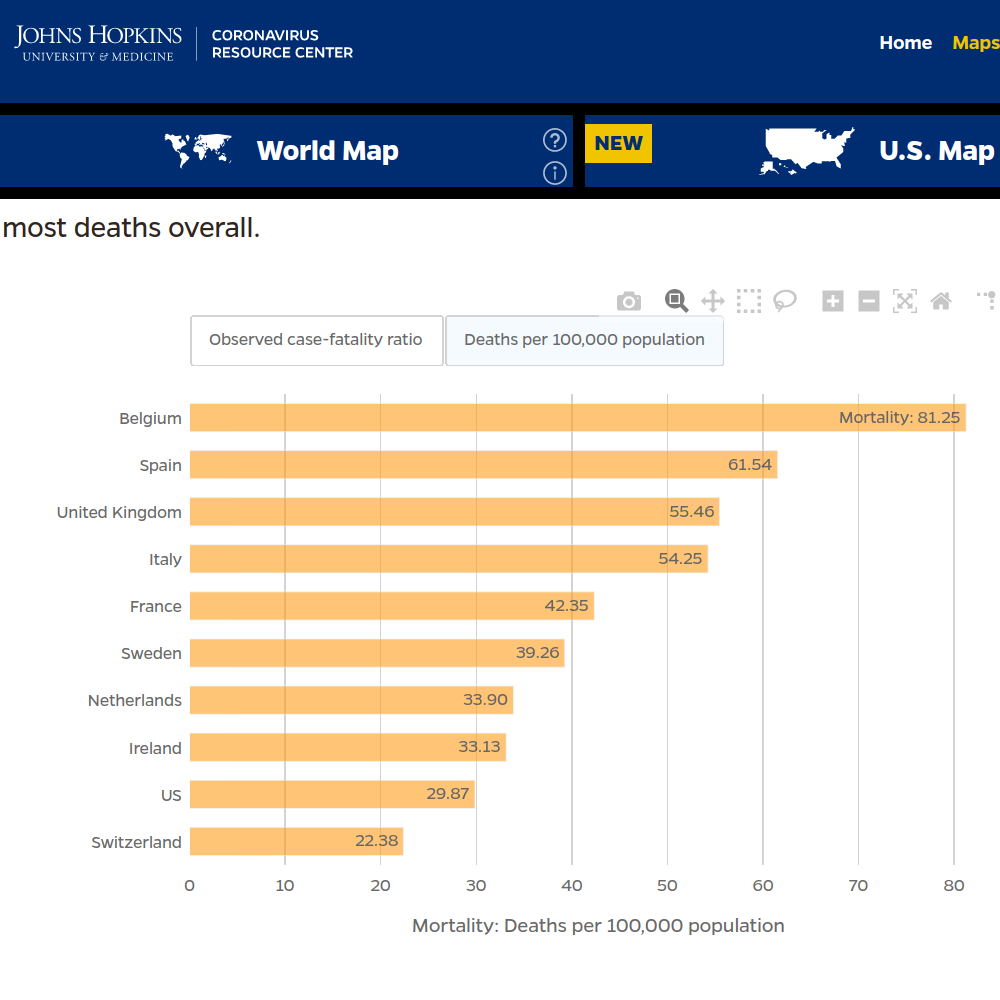
Source: https://coronavirus.jhu.edu/data/mortality
Looks like Norway, Finland, and Denmark (reporting 9.69 deaths per 100,000 on May 25, 2020) are so relatively low, they were not even included in the above data. Yet, all three countries surround Sweden.
.
If data presentation designed to perhaps inspire people to feel a certain way, or to believe a certain thing, is such a grievous occurrence, then who, pray tell, among us has “pristine and clean hands” ? 
Now this is rather “rich” (as they sometimes say). Here is the French press (France has a 7.87% higher incidence of COVID-19 deaths per 100,000 than Sweden) criticizing Sweden’s bold, hallowed approach:
(France 24, May 17, 2020):
“Sweden’s Covid-19 strategy has caused an ‘amplification of the epidemic’”
Sweden is famously one of the few countries to have opted against a lockdown to contain the spread of the coronavirus. But given that the country has a much higher death toll per million than its Nordic neighbours, many observers have suggested that the Swedish approach has failed. …
… Figures compiled by data analysis website Statista show that the total number of confirmed Covid-19 cases in Sweden has been increasing steadily since the beginning of April - and now stands at more than 29,000.
Statistics suggest that Sweden has performed poorly compared to its Scandinavian neighbours, which imposed strict lockdowns. Experts say the other Nordic countries are the most apt points of comparison, given their similar healthcare systems, socio-political cultures and levels of connected-ness.
Reported coronavirus deaths per million in Sweden stand at 358, according to Statista - even higher than the hard-hit US, at 267. The Swedish figure is dramatically worse than those of Denmark (93), Finland (53) and Norway (44). In Sweden, “we’re seeing an amplification of the epidemic, because there’s simply more social contact”, said Lynn Goldman, dean of the Milken Institute School of Public Health at George Washington University in the US. …
… Many Swedish experts have lambasted the government’s response to the pandemic. … As in many other countries, nursing homes have been a particular source of anguish. Although visits were banned on March 31, half of those 70 and older in Sweden who have died from Covid-19 were living in nursing homes, according to figures released at the end of April. Staff have warned that they lack personal protective equipment. …
… “There are things which could have been done, and should be done, that would have altered the picture radically,” said Lena Einhorn, a Swedish virologist and critic of the government’s policy. If Sweden had implemented “a broad testing programme, and especially in elder care”, she continued, the authorities would have “known who is infected, and now, with antibody testing, who was infected”.