They’ve known for a long time hydroxyhcloroquine and chloroquine aren’t like tylenol or an otc medicine. They’ve known of it’s heart issues since the 60’s? (rough guesstimate there). It’s potent. so is a Z-pack. I still don’t see the correlation between using the 2 together? The CDC and what Dr’s are saying that it does something completely different. They have known what it does to the heart though.
1 Like
Azithromycin is active (only) upon Bacterial organisms - period. Full stop. Various pneumonias are either caused by - or allow opportunistic Bacterial infections to take hold. Noting that the SARS-CoV-2 antigen is a Virus, we can therefore understand that Azithromycin in fact does not treat COVID-19 itself (without Bacterial activity). Seems like these facts ought to clear things up as to what is going on there.
1 Like
@Raven-Knightly
It’s beginning it’s continental adaptations That’s to be expected. Now the original strain and the hybrid will begin to compete with the original strain… That’s when one of them becomes a monster compared to what we have. Simple law… survival of the fittest. It looks like we have a new bug becoming prominent They need something to knock them both out at the same time.
1 Like
You are sort of sounding like a Cannabis aficionado there. Perhaps CBDs are the answer, Doctor ? ![]()

2 Likes
3 Likes
@Raven-Knightly
If you look at the side effects of both I wouldn’t be surprised if both could damage hey heart. They have to know that’s a pretty dangerous combo go give because each on it’s own is pretty rough by themselves. One could follow another possibly to reduce the threat of that occurring.
1 Like
If one has a bacterial infection, then it either needs treatment - or not. Azithromycin (also) has some small number of persons in whom it caused (delayed) severe Liver failure. If/when one is at super low Oxygen levels, on their back, and all pumped with various compromising chemicals, as well as heavily sedated due to intubation, that is a bad time to “push the envelope” of systemic/internal-organ toxicities.
1 Like
(South China Morning Post, April 14, 2020):
“The coronavirus mutation that threatens the race to develop vaccine”
1 Like
Text below is excerpted from the above-linked South China Morning Post article:
The researchers - led by Wei-Lung Wang, from the National Changhua University of Education in Taiwan, and collaborators from Murdoch University in Australia - said this was the first report of a significant mutation that could threaten development of a vaccine for the virus that causes Covid-19.
“The observation of this study raised the alarm that Sars-CoV-2 mutation with varied epitope [something an antibody attaches itself to] profile could arise at any time,” they wrote in a paper released on preprint review site biorxiv.org on Saturday. “[This] means current vaccine development against Sars-CoV-2 is at great risk of becoming futile.”
1 Like
(CNBC, April 13, 2020):
“WHO officials say it’s unclear whether recovered coronavirus patients are immune to second infection”
… A preliminary study of patients in Shanghai found that some patients had “no detectable antibody response” while others had a very high response, said Dr. Maria Van Kerkhove, WHO’s lead scientist on Covid-19. …
… “There are many reasons why we might see reactivation of infection either with the same infection or another infectious agent,” he said. In general, “there are many situations in viral infection where someone doesn’t clear the virus entirely from their system.” Some patients can also clear the main infection but develop a secondary bacterial infection, he said. …
… “While Covid-19 accelerates very fast, it decelerates much more slowly. In other words, the way down is much slower than the way up,” WHO Director-General Tedros Adhanom Ghebreyesus said at a press conference at the organization’s Geneva headquarters on Monday. “That means control measures must be lifted slowly and with control. It cannot happen all at once.”
1 Like
(Science Magazine, April 8, 2020):
“For survivors of severe COVID-19, beating the virus is just the beginning”
COVID-19’s immediate assault on the body is extensive. It targets the lungs, but a lack of oxygen and widespread inflammation can also damage the kidneys, liver, heart, brain, and other organs. … Although it’s too early to say what lasting disabilities COVID-19 survivors will face, clues come from studies of severe pneumonia - an infection that inflames the air sacs in the lungs, as COVID-19 does. Some of these infections progress to acute respiratory distress syndrome (ARDS), in which those sacs fill with fluid. That condition sometimes leads to scarring that can cause long-term breathing problems, Ferrante says, but studies show that most ARDS patients eventually recover their lung function.…
… Many COVID-19 patients who need a ventilator never recover. “What we’re finding in COVID is that there’s a ton of delirium,” says E. Wesley Ely, a pulmonologist and critical care physician at Vanderbilt University whose team is preparing to publish those findings. The virus itself is partly to blame, Ely says. He suspects this coronavirus, like the ones that cause severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome, can directly infiltrate and damage the brain. And bodywide inflammation caused by the virus can also limit blood flow to the brain and kill brain cells.
2 Likes
Nah, I’m enjoying my child’s learning at home. She is, too. Our original plan, when she was about to start school was home schooling.
We gave her the choice, when she was 6, to either go to school or homeschool. She chose to go to standard school.
She’s now realizing she should have chosen homeschooling…lol
3 Likes
Went out today. Took my tax information to the accountant, kinda… Slipped it under the door. They are working from home. The streets were pretty barren as were most businesses. Sandy went with me and went shopping at Kroger’s for a friend that is running out of money. Got a Dairy Queen Ice cream thing. Stopped at Office Max for more school supplies for children. It was totally weird out there. Nothing but the wind.
3 Likes
Pretty vague report - as is the somewhat clinically abstruse (“diagnostic”) term “schizophrenia”. The human factor in making such declarations of this or that “mental disorder” (without any particular clinical physiological metric) makes studies based on (possibly) shaky initial premises problematic. (Of course), people are anxious, perhaps panicking, and depressed due to the current psycho-social environment(s).
I saw that (what appears as mere) speculation, as well. There exist but a few entry points into the cerebral blood-brain-barrier where foreign microbes (might, possibly) find a way through into the brain.
It appears that the effects upon the Heart (and consequentially Kidneys and possibly Liver) are likely potentially beyond that of the lungs pulmonary output, however. The ACE2 Receptors that SARS-CoV-2 binds to are part of the regulatory “renin-angiotensin system”). (Some) patients have been reported with having COVID-19 cardiovascular (as opposed to the more common pulmonary) symptoms, primarily.
I previously posted a link or two of research communications (above in this thread). Here are two:
.
Persons having pre-existing (including so far un-diagnosed) issues and conditions surrounding cardiac (heart) functionality are advised to have a look at this info. This appears to be a genuine concern:
https://www.nytimes.com/2020/03/27/health/coronavirus-cardiac-heart-attacks.html
(JAMA, March 27, 2020): “Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19)”
I know it was vague. I was waiting for you to fill in the blanks. ![]()
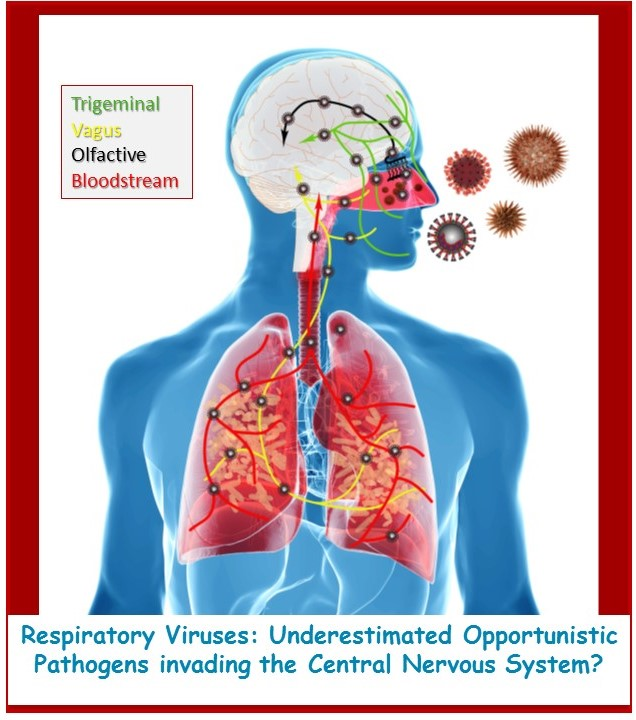
The question that arises is how respiratory viruses can be effective in the etiopathology of neuropsychiatric disorders.
https://www.sciencedirect.com/science/article/pii/S0165178120306089?via%3Dihub
1 Like
Mew, as you may have possibly sensed, I don’t particularly hold the field of psychiatry in high regard (with, IMO, some compelling reasons). Such irreverence must surely be some declared and named “disorder” (“Borderline Anti-Social Personality Dysmorphia” ?) I patiently await my “official diagnosis”.
Found the abstract for the single relevant (referenced) publishing here. When question marks appear after statements, I reason that such humility surrounding speculations likely implies, “definitely maybe”.
The abstract states:
For a few decades now, data reported in the scientific literature has also demonstrated that several respiratory viruses have neuroinvasive capacities, since they can spread from the respiratory tract to the central nervous system (CNS).
I note the use of the terms, “could”, and “may”:
Viruses infecting human CNS cells could then cause different types of encephalopathy, including encephalitis, and long-term neurological diseases. Like other well-recognized neuroinvasive human viruses, respiratory viruses may damage the CNS as a result of misdirected host immune responses that could be associated with autoimmunity in susceptible individuals (virus-induced neuro-immunopathology) and/or viral replication, which directly causes damage to CNS cells (virus-induced neuropathology).
The etiological agent of several neurological disorders remains unidentified.
Source:
https://www.mdpi.com/viruses/viruses-12-00014/article_deploy/html/images/viruses-12-00014-ag.png
Unfortunately, the published abstract is not accompanied by references to any relied-upon sources.
.
Not to say that human physiology intertwined with (subjective by nature) “psychological observations” is not an interesting (albeit super complex and implicitly problematic, and presenting some astronomical barriers to averments of so-called “scientific” understandings) subject-area. A lovely ethical mine-field.
(CNN, April 14, 2020):
“Prominent scientists have bad news for the White House about coronavirus antibody tests”
…There are several layers of issues with the antibody tests. First, the US Food and Drug Administration relaxed its rules, and now companies can sell antibody tests without submitting validation data that shows they actually work. The American Public Health Lab Association says that has resulted in “crappy” tests flooding the market. … There has been concern that some of the tests might confuse the coronavirus causing the current pandemic with one of several coronaviruses that cause the common cold. “Lots of tests confuse the two,” Relman said. The tests would then end up telling people they had antibodies to the pandemic coronavirus when they didn’t, and people might think they’re immune when they’re not. …
… Results from antibody tests “should be viewed as suspect until rigorous controls are performed and performance characteristics described, as antibody detection methods can vary considerably, and most so far have not described well-standardized controls,” according to the letter. Second, there are good tests in the midst of the bad ones, but they’re not yet widely and easily available throughout the country. Third, it’s not entirely clear that having antibodies to Covid-19 means that you truly have immunity and won’t get the disease again.
(France24, April 11, 2020):
“Coronavirus found in air samples up to 13 feet from patients”
.
(Fox News, April 10, 2020):
“Chilling video reveals how coronavirus spreads from a single cough in a supermarket”